
- How banning a TB test will save lives in India – “India, which each year has two million new cases of tuberculosis—the largest number in the world—has become the first country to ban the dangerously misleading blood tests that have long been the country’s cheapest and most ubiquitous diagnostic tools.” From Emory.
- No kids for me, thanks: I tied my tubes at 26 – And she had to lie to a doctor to get that tubal ligation after another doctor backed out. From Donnie.
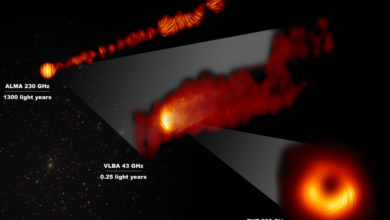
- Hot physics gossip suggests Higgs Boson discovery next week – It’ll be interesting to see how it gets reported on.
- The only good abortion is my abortion – Heartbreaking and angering at the same time. From Kirsten.




Never read the comments, but in the Higgs article, there are bunch of really good, if snarky, responses to the “who cares” comments. I especially liked the one about research on hamster gut flora, even if presumes speculative facts. (But confirming or disproving that kind of speculation is what science is all about.)
P.S. The sponsored ad above is for “free Tide Pods”. I misread it at first as an ad for free tide pools, and was really disappointed.
So, I responded to a post of this on G+ (Jennifer Ouellette’s stream) with…
You know why I’m pro-choice? I’m pro-choice because of my mom.
My mom was married in ’71; my brother followed two years later. My younger brother was planned… just was born about a year before he was planned. After that, Dad got snipped. So, to the best of my knowledge (having not inquired too closely into their pre-marriage sex life), abortion was never a personal issue for her.
But she was in school before Roe v. Wade. And she did see people she knew who tried a lot of different ways to abort fetuses they didn’t want. Coat-hangers. Lye. Things that fucked them up pretty damn good, when they worked.
Banning legal abortions does not prevent abortion… it prevents legal abortions. It prevents safe abortions. And I haven’t heard a response to this aside from variations on “suck it up and deal”.?
The only good abortion is my abortion
This is exactly what my wife and I went through. Mostly her. This is why I have no patience for people who want to outlaw D&C. It is a medical procedure not a moral statement. Without this option, which in no way killed a viable fetus, she just would have had to wait around for a miscarriage that may or may not have happened. I cannot imagine many things more horrible.
Abortion is rarely easy for anyone involved- the patient, the provider, the OR staff- no one enjoys having/doing them. It’s why I always tell med students who rotate with me that they should at least be in the room for a termination- to see that it’s not something that we enjoy doing but something we do to help and serve our patients. Most of them actually gain better perspective when they meet women who have struggled with the decision to terminate.
As for not tying a 26 year old’s tubes: I can understand that. The data show that many childless women under thirty who get a BTL regret the decision. With great long term contraceptive options (IUDs), in most cases patients fare better in the long term waiting for a tubal until later in life. That said, if very well counseled with excellent documentation, providers should respect a woman’s choice.
I’m a huge fan of IUD’s but some women just aren’t able to use them. Or a woman may not want either option currently available (at least in the US): hormones (though very low dose, obviously) or the heavy bleeding that can come with the copper IUD.
I agree that counseling should be given for any medical decision that has such a long term effect. However, are men who want vasectomies at 26 subjected to as much questioning as women who want tubals are? Are they often turned down and/or required to give extensive documentation at the rate that women are?
I can’t speak to vasectomy counseling because I haven’t had a male patient in years but I would hope it’s the same- it would be for me if I dealt with the men anyway. And as far as documentation, I meant the physician should document her ass off because law suits for regretted tubals are unfortunately too common and OB/GYN is a field full of litigation.
It is true that a fibroid uterus can prevent a successful IUD placement. Very rarely is a levonorgestrel IUD (Mirena) contraindicated. The hormone release is local and not systemic- there is, however, a relative contraindication with a current blood clot (but I wouldn’t operate on someone with an active clot either). That said, obviously women should talk to their doctors and give a complete medical history prior to any surgery/procedure/medication.
It’s NOT the same, and that’s her point.
Almost any man can walk in and get snipped, no questions asked. I’ve NEVER had ANY man (and I know quite a few who have been snipped) who have said that they had any trouble whatsoever.
But aside from my one friend, every other woman I’ve talked to has had issues getting a tubal.
If a woman gets a tubal and does not understand that it’s not reversible, that does not say to me that the women regretted her decision because she changed her mind — it says to me that she wasn’t properly educated in the first place and wasn’t made fully aware of some really important information. And that is a failure of the medical staff, not a failure of her.
Something tells me if 70% of your community regrets the tubal something is wrong with the medical community and how they are informing their patients, and it’s not just ‘cuz women are stupid and can’t make up their minds.
Also, we need to start trusting women. Yes, counseling is important, but you also have to just trust your patient after she’s made her decision, and after all counseling has occurred, and not try and lecture her about how she’s totally going to change her mind. Because I assure you, men are not treated in this manner. Women are treated in this matter because people assume that every woman will want — need — to have a kid, and that they don’t *really* understand what they are getting themselves into, and on top of that, many people believe women SHOULD have kids. A lot of this “but you’ll regret it!” is just projection of their own beliefs.
Full disclosure: I have NEVER refused a tubal for a woman 21 or older (Medicaid won’t pay for a tubal under age 21). I also promise that every patient is consented that this is a permanent procedure. Unfortunately, a medical degree and license are no match for “but my cousin’s friend’s aunt got hers reversed and had eight children”.
I also think you’re speaking from a privileged position. I don’t know your background but you seem like an intelligent, educated (whether formal or informal) woman who doesn’t easily succumb to pressure from her partner. Most of my CHS patients don’t meet this description and many of them are reacting to pressure from their partners/financial pressures. When these factors change five years down the line, there is sometimes regret. I think it’s fair to ask in detail what their motivations are and to ask them to consider their futures carefully.
I agree that women need to be trusted to make decisions- which is exactly what I do everyday providing the services we are talking about here. Part of that is asking lots of questions- you can’t say at first that we should treat female sterilization like we do male “no questions asked” then say that we “aren’t informing patients”. The reality is that young women of lower socio-economic status have a higher regret rate for LOTS of reasons, many of them out of the control of her provider. I have to BOTH ask lots of questions AND trust her decision which is sort of a damned if I do damned if I don’t situation based on what’s being said here.
I think we fundamentally agree on most things. I don’t support at all what happened to the woman in this article- and it wouldn’t have happened if I were her physician- but I am trying to provide perspective on why so many of us advocate the IUD- similar efficacy but less permanent for when life changes happen.
Don’t know about extensive documentation, but I have had one acquaintance report that the doctor refused to snip him since he was under 30 and had no kids.
Personally, I think the doctor would’ve done us all a favor if he’d smashed ’em with a rock while the dude was in local but, you know, doc wouldn’t do it for the $20 I had.
I know that when my now-husband whent to look into one at 25 they put up a decent bit of resistance at Planned Parenthood but eventually let him schedule an appointment after he had a consultation.
A friend of mine found an awesome doc and was given a tubal.
At 21 years old.
How this happened in Arizona of all places, I have no idea, but she’s resourceful and knows how to find really great doctors (her hubby is good at this too).
10 years later, at 30, and she is still happily child-free.
And I’ve had patients cry in the recovery room after a tubal because “I’ll never be a mother”. Ideally, patients are smart and educated about their options and their future plans. But especially in the underserved population I deal with, there is a common misconception that tubals are reversible. In our community health service population the regret rate for patients under thirty hovers around 70%. I think it’s resasonable to make sure patients understand very well what they are signing up for- especially if they don’t have the resources to pay for infertility treatments.
Admittedly, we are probably talking about apples and oranges because your friend doesn’t sound like my typical patient. Again, I can’t speak to vasectomies because I don’t do them or counsel for them so I’ll take you at your word that it’s easy to get one- a fact I find sort of disturbing. Although I wonder what percentage of men under 30 get a vasectomy compared to their female counterparts and BTLs.
Dammit lack of edit feature! I meant that I’ve had A patient (1) cry in recovery. It’s not common. I’m only pointing out that for every nullip that’s psyched about their tubal there’s a devastated one.
We shouldn’t use that information to limit women’s options, though.
This is basically the same kind of argument used by pro-choicers: “But they’ll regret it!”
So just keep that in mind. :)
When I woke up in the recovery room after my tubal, at age 24, I was laughing.
I’m now 35, and I couldn’t be happier with my decision. I haven’t had a nanosecond of regret. I’m forever grateful to my surgeon and to Planned Parenthood for helping me. They treated me with respect and care.
Also, you need to understand that even for women who are 100% positive about their decision may still feel very emotional directly after the fact. It’s a HUGE change and sometimes the finality hits you after the fact. I wouldn’t be surprised if a lot of those women remember *why* they made the decision in the first place, and don’t actually regret the decision, after some time has passed.
Just ‘cuz a woman is feeling very strong emotions about the procedure does not necessarily mean she regrets it.
It can also be hard to reconcile the social aspects of it. A lot of people consider women who can’t/don’t want to have children as “broken” or “wrong” and that can sometimes be hard to reconcile.
So unless you have some information for me regarding following up with these patients, I’m not really willing to believe that 70% of these women really, truly regret the decision.
That number is a follow-up number and is biased for a few reasons: 1) patient population as I talked about earlier. 2) in this same population it’s not uncommon for women to stop receiving health care unless they need it (ie loss to follow up for those who are happy and returning unhappy patients). I’m sure there are other reasons. The actual regret stats look like this
“Patient regret following the procedure is the most common long-term complication of sterilization, with rates reported anywhere from 0.9% to 26% for female sterilization32 and less than 5% for male sterilization.33 According to the CREST study, the cumulative probability of expressing regret following tubal sterilization was 12.7% (95% CI, 11.2–14.3).32”
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2492586/
Aaaand I just reread my first post and I now understand your response. I wrote that I could understand not tying a 26 year old’s tubes. I meant that I can understand encouraging less permanent options and having some discomfort HOWEVER in the end a well counseled woman’s choice needs to be respected. Sorry for the confusion. I guess reading what I write before hitting submit would be advisable. ;)
Displaced Northerner. I totally see your points re: socieconomcics and what not — and thanks for the figures and stuff, that helps!
Anyway, your last paragraph, basically, is how it should be done. That said, “encouraging less permanent options” can often come across as not respecting the choice of the women — so I think “encouraging’ is maybe the wrong word? I think maybe, “Educating women on all of their options and the negatives and positives of all options” is maybe better.
We shouldn’t “encourage” women to make certain choices. We should give them all the tools os they can make their own informed choices.
awkward sentence structure is maybe awkward